

Data
In this article
Monitor
An ongoing HIV epidemic
Nearly 170,000 people are living with HIV in France. In fact, the prevalence of the infection is estimated at approximately 0.4% among adults aged 15 to 49. The number of people discovering their HIV-positive status each year is estimated at approximately 6,200.
Approximately 6,200 people learned they were HIV-positive in 2019.
According to the WHO, the HIV epidemic in mainland France is considered concentrated. This means that it affects the general population very little but disproportionately affects certain population groups:
43% of people who learned they were HIV-positive in 2019 were men who have sex with men (MSM).
People from sub-Saharan Africa infected through heterosexual contact accounted for 37% of HIV diagnoses in 2019. People born in France infected through heterosexual contact accounted for 14% of diagnoses.
People who inject drugs (PWID) accounted for 2% of HIV diagnoses in 2019.
HIV testing activity and new HIV diagnoses were impacted by the COVID-19 pandemic. In 2020, 5.2 million HIV serology tests were performed by clinical laboratories. HIV testing activity, which had increased between 2013 and 2019, decreased between 2019 and 2020 (-14%).
The number of new HIV diagnoses in 2020 was estimated at 4,856 [95% CI: 4,481–5,231], representing a 22% decrease compared to 2019. This decrease in the number of HIV diagnoses can be explained in part by reduced testing activity. It could also be due to lower exposure to HIV linked to social distancing measures, which were most likely limited to the first lockdown.
Learn more:
Gonococcal infections that primarily affect men who have sex with men
In 2020, 2.1 million gonorrhea tests were performed by private laboratories and approximately 254,000 at CeGIDD. The number of gonorrhea diagnoses decreased by 13% at CeGIDD, and the positivity rate rose from 3.2% to 3.9%. This rate was higher among men (5.8%), particularly MSM, and transgender individuals (6.3%) compared to women (1.2%). The majority of patients diagnosed in primary care in 2020 were men (77%), 54% of whom were MSM.
Learn more: Gonorrhea thematic report
Syphilis infections that primarily affect men who have sex with men
In 2020, 2.4 million syphilis tests were performed by private-sector laboratories and approximately 2,500 at CeGIDD. The number of diagnoses decreased by 18% at CeGIDD, and the positivity rate rose from 1.2% to 1.4%. This rate was higher among MSM (2.4%), whether born in France or abroad, compared to heterosexual men (0.4%) or heterosexual women (0.3%). All patients diagnosed in primary care in 2020 were men, 85% of whom were MSM.
Learn more: Syphilis thematic report
Chlamydia trachomatis infection, diagnosed primarily in women and heterosexual individuals
In 2020, 2.3 million tests for Chlamydia trachomatis (Ct) infection were performed by private laboratories and approximately 258,000 by CeGIDD. Between 2019 and 2020, the number of Ct infection diagnoses decreased by 8% in the private sector and by 31% at CeGIDD. The positivity rate at CeGIDD remained stable over these two years, at around 7%. The majority of patients diagnosed in primary care in 2020 were women (54%) and heterosexual individuals (75%). Among Ct-positive anorectal samples analyzed in 2020 by the National Reference Center for Bacterial STIs, the prevalence of lymphogranuloma venereum (LGV) was 13.4%.
Learn more: Chlamydia thematic report
Measure
In the general population
Sexuality over the course of a lifetime
The 2016 Health Barometer provided an opportunity to assess changes in the sexual behaviors of the French population since the 2006 survey on the Context of Sexuality in France (CSF).
In 2016, the average number of sexual partners was 6.0 for women, compared with 4.4 in 2006 and 3.3 in 1992. For men, the increase was less pronounced: 11.0 in 1992, 11.6 in 2006, and 13.9 in 2016. While the gaps have narrowed slightly over time, the difference between the two sexes remains significant and partly reflects the fact that the definition of a sexual partner differs by gender.
The ways in which people meet partners have changed significantly between 2006 and 2016. Data from the 2016 Health Barometer show that the proportion of women and men who met a sexual partner online is increasing (9.3% of women in 2016 compared to 2.7% in 2006, and 14.6% of men in 2016 compared to 4.6% in 2006).
One of the most striking features of changes in sexual behavior over the past few decades has undoubtedly been the extension of sexual activity—particularly among women—beyond the age of 50, as shown by analyses of the 2006 CSF survey. This trend has, however, leveled off over the past decade. Women are less likely to live in a couple than men, due in particular to men’s preference for younger partners and higher male mortality rates. Women and men aged 50–69 who live in a couple do not report having more sexual intercourse today than in 2006 (86.7% vs. 90% for women; 92.7% vs. 95% for men). The gaps between women and men widen with age and are much more pronounced among those who do not live in a couple. Thus, 14.9% of women aged 70–75 who are not in a couple have had sex in the past twelve months, compared to 56.9% of men in the same age group.
Women report more frequently than men that their first sexual encounter was forced (1.7% versus 0.3% for men), with disparities based on sexual orientation.
Over the course of their lives, data from the 2016 Health Barometer show that 18.9% of women and 5.4% of men aged 18–69 report having experienced attempted or forced sexual intercourse. The extent of this phenomenon was more pronounced in 2016 than in 2006 for women (18.9% versus 15.9%), while reports from men remained at the same level as 10 years ago (5.4% versus 4.5%, a non-significant difference). The first experience of such violence occurs predominantly before the age of 18, in 47.4% of cases for women and 60.2% for men.
Changes in contraceptive practices
In 2016, 92% of women who needed contraception reported using a method to prevent pregnancy. The pill remains the most widely used method of contraception: 36.5% of women use it, with variations by age: 60% among those under 25, 48% among those aged 25 to 29, and 35% among those aged 30 to 34. Use of the pill declined following the discussions surrounding the “pill crisis” of 2012, but the proportion of women of reproductive age not using any form of contraception has not changed. The decline in pill use has shifted toward IUDs and condoms, with variations by age group. Starting at age 30, intrauterine devices (IUDs) replace the pill and are the most commonly used contraceptive, with more than one in three women using them. Across all age groups, IUDs are used more frequently by women with children than by nulliparous women. The hormonal implant, used by 4% of women, ranks third among the most frequently used methods, far behind the pill and the IUD. As with the IUD, the implant is primarily used by women who already have children. So-called natural contraceptive methods are used by less than 5% of women.
Contraceptive methods used in France in 2016 by women using contraception, by age
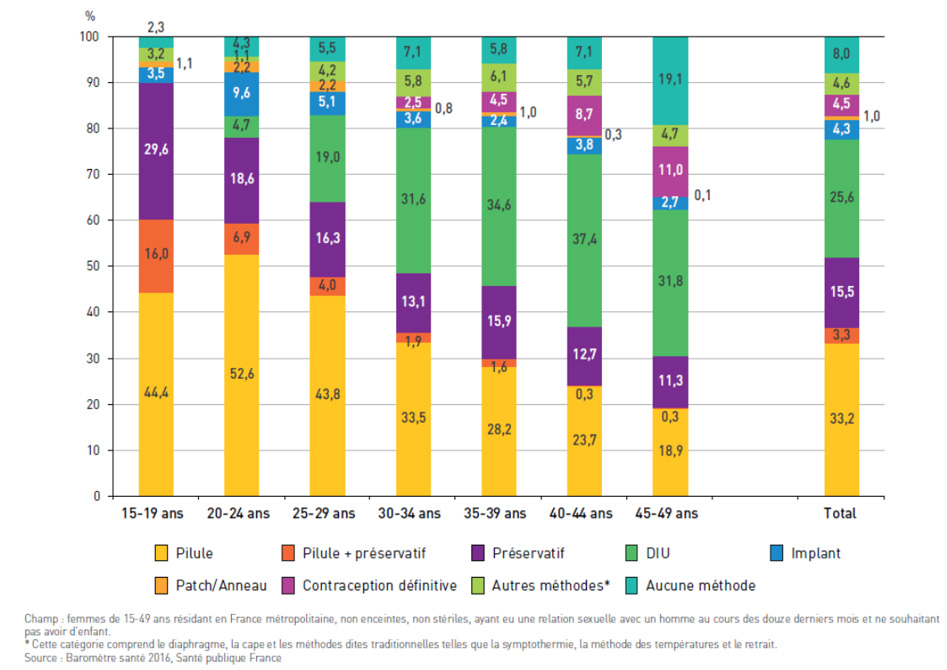
These figures show that contraception remains highly medicalized in France and continues to follow a pattern that establishes the condom as the method of protection during first sexual encounters, followed by the pill when entering a relationship, and then the IUD at childbearing ages. The use of methods such as the implant, the patch, or the ring remains low and is primarily limited to young women under 25.
Access to emergency contraception (EC) has changed since it first became available. It is now available without a prescription and without restrictions at pharmacies and from many healthcare providers. In 2016, 6.2% of women aged 15–49 who were at risk of an unintended pregnancy had used EC in the past 12 months. The youngest women, those living in the Paris region, and those using hormonal contraceptive methods whose effectiveness depends on regular use (the pill, patch, or ring) were the ones who used this backup method the most. Indicators of sexual risk-taking, such as reporting a sexually transmitted infection, an unintended pregnancy, or recent multiple sexual partners, were also associated with more frequent use of EC. Finally, there is a link between EC use and knowledge and perceptions. Women with a good understanding of the time limits for taking EC and those who perceived EC as effective reported using it more frequently.
Despite easier access and significant changes in the contraceptive landscape, the use of EC did not increase in France during the 2000s. Similarly, the profile of women who use it has changed little. The promotion of emergency contraception as a complement to regular contraception must be supported in a context where the number of unintended pregnancies and voluntary terminations of pregnancy remains stable.
In 2016, more than 95% of people under 30 reported being aware of emergency contraception, and 81.5% of people in this age group knew that it was available without parental consent. 82.1% of respondents were aware that emergency contraception can be purchased without a prescription directly at a pharmacy. Awareness of this information decreases with age, falling from 86.4% among those under 20 to 84.8% among those aged 20–24 and 75.8% among those aged 24–29. The fact that emergency contraception is free for minors is known by 86.5% of women and 79.3% of men aged 15–19.
Data regarding awareness of the time limits for use reveal a significant lack of information. The maximum time limit of 120 hours after sexual intercourse is cited by less than 1% of respondents. The 24-hour time limit is cited most often (39.2%), followed by the 48-hour limit (22.8%) and the 72-hour limit (16.8%). At the extremes, 14.0% of respondents state that EC must be taken within 24 hours of unprotected sex, and 3.2% that it can be taken more than 120 hours later. Women’s perceptions of the time window are closer to reality than men’s.
Abortions
Data from the Directorate for Research, Studies, Evaluation, and Statistics (Drees) show that 222,000 abortions were performed in 2020, representing a decrease of approximately 4% compared to 2019, primarily observed in mainland France. The COVID-19 pandemic and the measures taken to limit its spread had an impact on conceptions during the first lockdown, leading to a decrease in births observed in 2020, as well as a decrease in abortions. The abortion rate is declining in mainland France: in 2020 it stood at 14.9 per 1,000 women aged 15 to 49, compared to 15.6‰ in 2019. In the overseas departments and regions (DROM), it remained virtually stable: 28.4‰ in 2020, compared to 28.5‰ in 2019.
The year 2020 was marked by a significant decline in the number of abortions performed in healthcare facilities (154,000 compared to 170,000 in 2019), while non-facility medical abortions increased at the same rate as in previous years (67,800 compared to 62,000 in 2019). 72% of all abortions are medical, whether performed in a healthcare facility or not.
Regional disparities persist, with rates ranging from one to three times higher depending on the region. In mainland France, they vary from 11.4 abortions per 1,000 women in the Pays de la Loire region to 21.7 abortions in Provence-Alpes-Côte d’Azur. Corsica saw its rate of recourse decline more than other regions, and no decline was observed in the DROMs, where rates remain at or exceed those recorded in 2019, surpassing 39 per 1,000 in Guadeloupe and French Guiana.
The full results are available on the Drees website: Voluntary Terminations of Pregnancy: A Slight Decline in the Rate of Recourse in 2020.
Among young people
The age at first sexual intercourse has remained stable for the past 10 years
The age at first sexual intercourse stabilized between 2005 and 2016 and currently stands at 17.6 years for girls and 17.0 years for boys, with no notable difference based on socioeconomic background. The gap between girls and boys is about six months, as it was in the early 2000s. While girls and boys experience this particular event at roughly the same age, the characteristics of the partner and the expectations of young people indicate that the experience remains strongly gendered. Young girls are thus more likely to have their first sexual experience with a partner who is at least two years older (half of them compared to one-fifth of boys) and who has already had sexual intercourse. They are also less likely than men to begin their sexual lives before age 15 (6.9% vs. 16.5%). So-called “late” first sexual experiences, beginning at age 19 or older, account for 33.2% of women and 23.1% of men. No significant changes in these two indicators have been observed over the past four decades.
First sexual intercourse mostly desired, but not always
The vast majority of respondents report having wanted this first sexual encounter “at that time.” Nevertheless, slightly fewer women than men reported this (87.6% vs. 92.8%). Women were more likely to report having yielded to their partner’s expectations (10.7% vs. 6.9%) or even having been forced into the encounter (1.7% vs. 0.3%). While 53.6% of women cite love or tenderness as the reason behind their desire for their first sexual encounter, only 25.9% of men cite these factors as the most decisive. Men cite sexual desire above all else (47.0% versus 25.8% of their female counterparts).
First sexual encounters are mostly protected
These first sexual encounters are protected in the vast majority of cases. A condom was used in over 85% of cases, with no difference between women and men. However, condom use is lower among women who had their first sexual encounter after age 19 (70.3%) and among men who had theirs before age 15 (76.0%). More than one in three women (36.9%) report having used the pill at the time of their first sexual encounter, whereas only one in four men (23.5%) report that their partner was using it. This disparity, already highlighted in previous surveys, raises questions about the differing levels of involvement of women and men in contraceptive matters.
For more information on the results: Bajos N, Rahib D, Lydié N. Gender and Sexuality: From One Decade to the Next. Health Barometer 2016. Saint Maurice: Santé publique France, 2018. 6 p.
The 2018 EnCLASS survey report provides data on the romantic and sexual relationships of middle and high school students.
The results, which describe the expression of romantic feelings, the circumstances surrounding first sexual intercourse, and trends observed over the past decade, are available on the EHESP website.
Among men who have sex with men
Regular HIV testing is a major public health issue, particularly among men who have sex with men (MSM), who remain one of the populations most affected by HIV.
The data are drawn from the two editions of the Enquête Rapport au Sexe (ERAS), from 2017 and 2019, indicate that the proportion of respondents who had never taken an HIV test in their lifetime decreased significantly from 17% to 15% in 2019, while testing in the past twelve months increased (from 53% to 55%). The proportion of respondents in 2019 who had taken three or more tests also increased, rising from 15% to 20%, regardless of the respondents’ characteristics. The use of Pre-Exposure Prophylaxis (PrEP) contributes significantly to this increase, given that the monitoring protocol requires HIV testing every three months. However, this upward trend is also observed among MSM who do not use PrEP.
The continuation of testing promotion campaigns targeting the MSM population in all its diversity, coupled with the implementation of a proactive, region-specific policy, are essential drivers for curbing the HIV epidemic.
The variety of testing methods available to users contributes to increased testing frequency. Thus, in 2017, 5.0% of MSM who responded to ERAS reported having used a self-test during their most recent HIV screening. These MSM had very different profiles: young men who had never been tested but were interested in non-medical testing tools, men reporting high levels of sexual activity who were already familiar with testing, and MSM reluctant to visit health centers.
These results demonstrate the value of this tool and support for its wider availability within the French testing system.
Learn more:
Velter A, Duchesne L, Lydié N. Increase in repeated use of HIV testing among men who have sex with men in France between 2017 and 2019. Results of the Rapport au sexe survey.
Lydié N, Duchesne L, Velter A. Who are the users of self-testing among men who have sex with men in France? Results of the 2017 Rapport au sexe survey. Bull Epidémiol Hebd. 2018;(40-41):800-5.
Protection against HIV during sexual intercourse is no longer limited to condoms alone; prevention has been expanded to include biomedical approaches such as TASP (Treatment as Prevention) and PrEP (Pre-Exposure Prophylaxis).
The results of ERAS 2017–2019 show that the overall level of protection during the most recent sexual encounter with a casual partner increased among HIV-negative respondents, rising from 74.1% to 76.5%. Condom use remains the most common practice but decreased between 2017 and 2019 (67.5% vs. 61.3%) in favor of PrEP use, which rose from 5.4% in 2017 to 14.0% in 2019. The likelihood of using PrEP during the most recent sexual encounter with a casual partner among HIV-negative MSM tripled between 2019 and 2017, all other factors being equal.
For more information: Duchesne L, Lydié N, Velter A. Increase in the overall level of protected anal sex among men who have sex with men in France: results from the repeated cross-sectional survey Rapport au Sexe, France, 2017–2019. AIDS Care. 2020;32(sup2):162–9.
More than a decade ago, the preventive effect of antiretroviral treatment for HIV, known as “TasP,” was scientifically proven: an HIV-positive person on treatment with an undetectable viral load cannot transmit the virus.
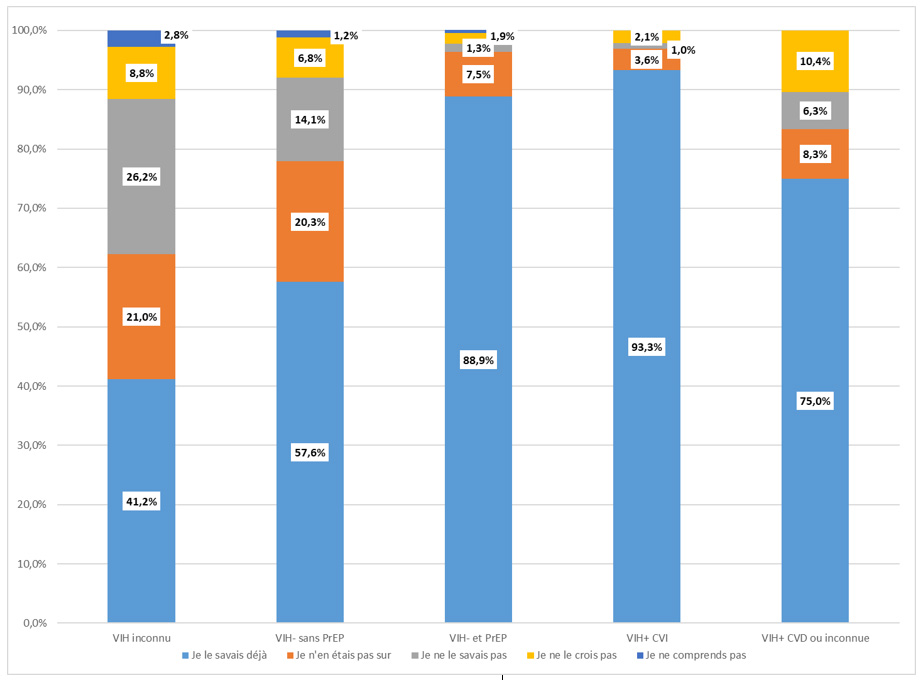
Data from ERAS 2021 show that awareness of this preventive tool remains insufficient among the MSM population: 60.5% of respondents are aware of TasP. This awareness level rises to 92.4% among HIV-positive MSM, while it stands at 58.2% among HIV-negative MSM or those unaware of their HIV status.
Distribution of responses to the question: "Before today, were you already aware of this information?"
"A person with HIV taking effective treatment (and with an undetectable viral load) cannot transmit the virus during sexual intercourse," according to the reported biomedical status. 2021 Sex Survey, France, n=14,706
For more information: Velter A, Ousseine Y, Allaire C, Lydié N. Awareness of the preventive effect of antiretroviral therapy (TasP) among men who have sex with men in France in 2021 – Results of the Rapport au sexe survey. Bull Epidémiol Hebd. 2021;(20-21):378-87.
A special COVID-19 edition of the ERAS survey revealed that lockdown measures had a negative impact on the living conditions of MSM, just as they did for the general population, with some experiencing a deterioration in their economic situation, substance use, or mental health. Regarding the continuity of care for other health issues, 35% of respondents forwent medical care and 28% postponed their HIV/STI testing. More than one-third of HIV-positive MSM postponed an HIV follow-up appointment.
In terms of sexuality, 60% of respondents did not have sex with casual partners. Among users of pre-exposure prophylaxis (PrEP), 59% stopped taking it due to a decrease in sexual activity, indicating compliance with social distancing measures but also the abrupt interruption of sexual socializing.
The health crisis highlights the specific pre-existing health vulnerabilities of gay and bisexual men: isolation, mental health, and substance use, compounded by socioeconomic vulnerabilities.
Learn more: Velter A, Champenois K, Rojas Castro D, Lydié N. Perceived impact of the COVID-19 pandemic on men who have sex with men in France. Bull Epidémiol Hebd. 2020;(33-34):666-72.
In 2015, HIV prevalence was estimated at 14.3% [95% CI: 12.0–16.9] among MSM frequenting gay social venues in Nice, Montpellier, Lyon, Lille, and Paris. HIV prevalence varied by city.
HIV Prevalence by City - Prevagay 2015, weighted data
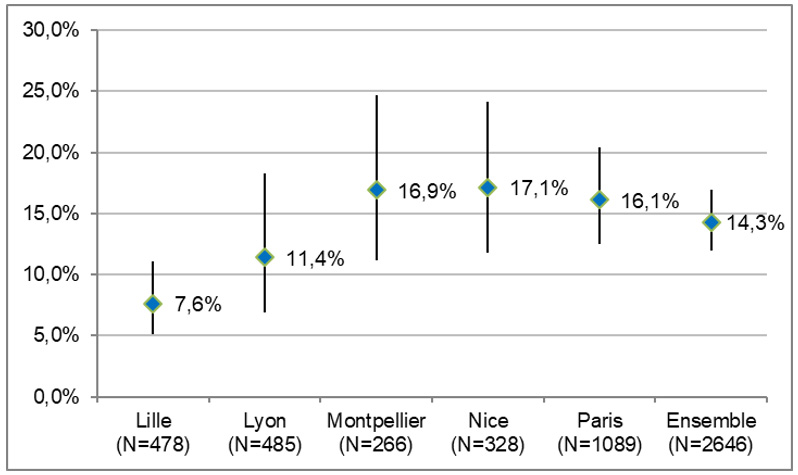
The estimated prevalence increased with age, rising from 6.5% (95% CI [4.1–10.1]) among men under 30 to 18.6% (95% CI [14.3–23.9]) among those aged 45 and older (p<0.03).
The proportion of diagnosed HIV infections among all MSM who tested positive was 90.5% (95% CI [84.5–94.4]), with no significant difference by city. The median time since HIV diagnosis reported in the questionnaire was 10 years (IQ 4–18). The proportion of HIV-positive MSM on antiretroviral therapy was estimated at 94.9% (95% CI [91.9–96.8]), with no significant difference across cities.
For more information: Velter A, Sauvage C, Saboni L, Sommen C, Alexandre A, Lydie N, Peytavin G, Barin F, Lot F. Bulletin Epidémiologique Hebdomadaire, 2017, No. 18, pp. 347–54
The "Presse Gay" surveys conducted between 1985 and 2011 provide insight into how the sexual and preventive behaviors of men who have sex with men (MSM) have evolved over a 25-year period. Generational analyses of the survey participants offer valuable insights.
Younger generations were more likely to have their first sexual experience with a man than previous generations: 84% of those aged 18 between 2008 and 2011 reported having had their first sexual encounter with a man, compared to 76% of those aged 18 between 1956 and 1959. The median age at first sexual intercourse with a man remained stable across generations at around 18 years. In terms of sexual practices, compared to their elders, younger generations reported engaging more frequently in oral sex and anal intercourse, but having fewer male sexual partners in the past 12 months.
These surveys also highlighted major changes in condom use among MSM over the past two decades. Thus, between 1991 and 1997, a decline in the proportion of unprotected anal intercourse with casual partners was observed.
Starting in 1991, this proportion increased from 13% to 25% in 2011 for HIV-negative MSM, and from 25% to 63% for HIV-positive MSM over the same periods. Regardless of respondents’ HIV status, this trend toward increased condom non-use is similar across all generations, indicating the influence of context on sexual behavior.
Learn more:
Methy N, Velter A, Semaille C, Bajos N. Sexual behaviors of homosexual and bisexual men in France: a generational approach. PLoS One. 2015;10(3):e0123151.
Methy N, Meyer L, Bajos N, Velter A. Generational analysis of trends in unprotected sex in France among men who have sex with men: The major role of context-driven evolving patterns. PLoS One. 2017;12(2):e0171493
Pre-exposure prophylaxis, or PrEP, is a prevention strategy in which a person who is not infected with HIV takes antiretroviral medications to prevent HIV transmission. In France, it has been available since January 2016. It is a powerful tool for significantly curbing the HIV epidemic among MSM (men who have sex with men).
The three editions of the Sexual Behavior Survey conducted in 2017, 2019, and 2021 among MSM shed light on trends in its use. Thus, among the 15,506 HIV-negative MSM respondents who reported having engaged in anal intercourse during their most recent sexual encounter with a casual partner, a significant increase in PrEP use was observed. The rate rose from 6.0% in 2017 to 15.7% in 2019, reaching 25.0% in 2021. However, the level reached in 2021 remains insufficient and requires continued information campaigns while improving access to this effective prevention tool.
Among migrants
Sexual and preventive behaviors among populations from sub-Saharan Africa and the Caribbean living in the Île-de-France region
In 2016, the AfroBarometer cross-sectional survey collected biological and socio-behavioral data from 1,283 Afro-Caribbean participants residing in the Île-de-France region. The majority of these participants were born in sub-Saharan Africa (64%), and half were between the ages of 18 and 34.
A fingerstick blood sample collected from the participants revealed an HIV prevalence of 1.6% among all participants and 15% in the subgroup of men who had exclusively had homosexual intercourse in the past 12 months. Of the 21 HIV-positive individuals, more than one in three was unaware of their HIV status (7 men and 1 woman). The blood test also revealed that 5.1% of participants were HBsAg-positive, a marker of acute or chronic hepatitis B virus infection. Among these individuals, more than three-quarters (77%) were unaware of their infection. These figures show that HIV and HBV testing rates are insufficient among the Afro-Caribbean population in the Île-de-France region. It appears essential to expand testing services beyond current testing facilities and to promote the distribution and use of rapid diagnostic tests that combine screening for HIV, hepatitis B, and hepatitis C, coupled with clear and tailored information and counseling.
The 2016 AfroBarometer showed that Afro-Caribbean populations remain a priority in the fight against AIDS. The prevalence observed among men who have sex with men (MSM), a group long overlooked, calls for urgent action. While the introduction of rapid HIV tests has increased screening rates in these populations, hepatitis B is also a major public health issue in terms of both screening and care.
For more information: Larsen C, Limousi F, Rahib D, Barin F, Chevaliez S, Peytavin G, et al. HIV and HBV infections among Afro-Caribbean people in Île-de-France: high prevalence and insufficient screening. Bull Epidémiol Hebd. 2017;(28-29):609-16.
As the first large-scale quantitative survey conducted among immigrants from sub-Saharan Africa, the ANRS Parcours survey provided an opportunity to describe and analyze the migratory, social, administrative, and health trajectories of this population in the Île-de-France region.
The primary finding of this survey was that the settlement process takes time: women wait six years and men seven years to gain access to stable housing, a residence permit valid for at least one year, and paid employment—the minimum conditions for settling in France.
Periods of precariousness are therefore common: one in two people lived for at least one year without a residence permit, and one in three lived for at least one year without stable housing; 14% of men and 5% of women had to sleep on the street at least once. Individual characteristics offer little protection against the risk of experiencing precariousness in France, which is largely due to structural factors, economic crises, and the tightening of immigration policies.
The periods of precariousness created by these initial challenges expose individuals to sexual risks and HIV infection. Women in particular are exposed to forced sexual relations and violence when they lack personal housing. Between one-third and one-half of immigrants from sub-Saharan Africa living with HIV in France were infected after their arrival (30% for women, 44% for men).
Once in France, access to HIV testing is relatively quick but remains insufficient overall. Half of African immigrants undergo an HIV test within two years of arrival. However, this is still not fast enough to maximize benefits for those infected or to achieve a significant preventive effect of treatment on the dynamics of the epidemic. Hepatitis B screening is not offered frequently enough: while it is known that approximately one in 10 adults in this population is a chronic hepatitis B carrier, men wait a median of four years to access it (it is faster for women, who are routinely screened during pregnancy). Once the infection is detected, access to care is rapid. Screening therefore remains the main weak point in the medical management of HIV and hepatitis B.
Beyond HIV and hepatitis B, the Parcours study provided insights into various aspects of the health of Africans in France. While alcohol and tobacco use appeared to be much lower in this group than in other segments of the French population, other indicators of poor health were observed: frequent symptoms of anxiety and depression (present in 25% of women and 18% of men); a high prevalence of overweight and obesity (51% among men, 68% among women), which carries cardiovascular risks.
This research has provided insights into the reception of immigrants in France and its impact on their health, particularly their increased vulnerability to HIV due to reception conditions. Continuing the prevention policies implemented over many years, while also improving reception conditions and better informing new arrivals about the social and health resources available to protect them from extreme precariousness—particularly homelessness—are thus public health imperatives. Safeguarding the healthcare and health insurance system, which protects the most vulnerable, even when they are undocumented, is a key component of this reception.
All results of the Parcours study are available here: https://www.ceped.org/parcours/
Try it out
The BaroTest demonstrated good acceptability and feasibility of self-collection using blotting paper among the general population.
The kit was accepted by 73.4% of participants and returned by one in two people, resulting in an overall participation rate of 37.0%. These rates are identical among men and women, but the factors associated with kit acceptance and sample return differ. Nearly 99% of the blotters received could be tested for the three infections.
The prevalence among 18- to 75-year-olds was estimated at 0.30% (95% CI: [0.13–0.70]) for chronic hepatitis C (CHC) and 0.30% [0.13–0.70] for chronic hepatitis B (CHB). The estimated proportion of infected individuals aware of their status is 80.6% [44.2–95.6] for CHC and 17.5% [4.9–46.4] for CHB. Universal combined HCV/HBV/HIV screening would involve testing 32.6% of this population, considering individuals who have not undergone any of the three tests, and 85.3% when also accounting for those already tested for one or two of the viruses.
The results of this study are available in the following articles:
Rahib D, Larsen C, Gautier A, Saboni L, Brouard C, Chevaliez S, Barin F, Lot F, Lydié N. Acceptability and feasibility of home self-collection testing for HIV, HBV, and HCV infections in the general population in France in 2016: the BaroTest study. Weekly Epidemiological Bulletin, 2019, No. 24-25, pp. 478-490.
Saboni L, Brouard C, Gautier A, Chevaliez S, Rahib D, Richard JB, Larsen C, Sommen C, Pillonel J, Lydié N, Lot F. Prevalence of chronic hepatitis C and B, and history of screening in the general population in 2016: contribution to a new screening strategy, Santé publique France Barometer - BaroTest. Weekly Epidemiological Bulletin, 2019, No. 24-25, pp. 469-477.
Brouard C, Saboni L, Gautier A, Chevaliez S, Rahib D, Richard JB, Barin F, Larsen C, Sommen C, Pillonel J, Delarocque-Astagneau E, Lydié N, Lot F. HCV and HBV prevalence based on home blood self-sampling and screening history in the general population in 2016: contribution to the new French screening strategy. BMC Infectious Diseases, 2019, vol. 19, no. 1, pp. 1–14.
In addition, the BaroTest 2016 protocol was published in English: Lydié N, Saboni L, Gautier A, Brouard C, Chevaliez S, Barin F, Larsen C, Lot F, Rahib D. Innovative Approach for Enhancing Testing of HIV, Hepatitis B, and Hepatitis C in the General Population: Protocol for an Acceptability and Feasibility Study (BaroTest 2016) JMIR Res Protoc 2018,7(10):e180.
During the four-week study period, 11,075 people were enrolled, 53% of whom were women. The average age of the participants was 20.7 years. About half were students, 20% were employed, and 14% were job seekers.
The percentage of people tested at the end of the study was 8.6% in the control group and 29.2% in the intervention group. Thus, sending a self-collection kit increases Chlamydia testing rates among young people by a factor of 3.4, with a greater multiplier effect among men than among women.
Sending a kit increases testing uptake across all population subgroups, except among women of Maghreb origin. It also helps reduce geographic inequalities in access to testing.
The positivity rate was 6.8%, higher among women (8.3%) than among men (4.4%). This rate is close to that recorded in the surveillance network (7%) but higher than the prevalence estimated in 2006 in the general population (between 1% and 3%).
Positivity rates were particularly high among men and women with multiple sexual partners (rates of 10% or higher). It should also be noted that positivity rates were between 1% and 3% among individuals generally considered low-risk because they reported having only one sexual partner during the year.
The economic analysis estimated the cost per person who underwent screening via self-collection at €32, compared to €73 for screening in the traditional system, a difference of €41. Further analyses are nevertheless needed to determine the cost-effectiveness of this approach.
The results of this trial are described in the following articles:
Used by nearly 30% of the men to whom it is offered, the self-collection kit helps bring a diverse population into the screening process, both in terms of sociodemographic characteristics and attitudes toward screening
Recruitment for the MémoDépistages study took place online from April 11, 2018, to June 10, 2018. The kit was offered to 7,158 men, and 3,428 (50%) agreed to receive it. These were young men at risk for STIs (high number of sexual partners, insufficient protection) and under-tested (only half had been tested in the past 12 months). Nearly 6 out of 10 men (58%) returned their samples to the laboratory. In total, nearly 30% of the men who were offered the kit were tested using the self-collection kit. These were predominantly urban men with a high level of education who were familiar with gay social venues. It was primarily sociodemographic factors (age, level of education) that were associated with a high rate of self-sampling use in the study.
The vast majority of kits received by laboratories were complete and usable for HIV testing (80%). For chlamydia (CT) and gonorrhea (NG) infections, over 99% of samples could be analyzed.
The rate of detection of new HIV infections was 0.5% (0.7% in the Île-de-France region). The overall positivity rate for CT was 9.3%, with the highest positivity observed in the rectal region (7.3%). For 80% of men testing positive for CT, the infection was isolated in the extragenital area and would not have been detected by a urine test alone. The positivity rate for NG was 9.6%, with the highest positivity observed in the pharyngeal area (7.2%). For 94.6% of men who tested positive for NG, the infection was isolated in the extragenital region and would not have been detected by a urine test alone. In total, 17.1% of our sample tested positive for CT or NG at at least one sampling site.
For the reporting of positive results (including HIV), men chose, in order, a phone call, a text message (which informed them that their results were available), and a doctor.
All HIV-positive results were delivered by phone, which facilitated the connection to care and management for those diagnosed. Following this initial test, 68% of participants scheduled a follow-up test in three months.
The results of this pilot study are available in the following publications:
Rahib D, Delagreverie H, Gabassi A, Touré T, Le Thi T, Vassel E, et al. Profile of users of the first self-sampling screening kit from the MémoDépistages program offered to MSM with multiple partners in France in 2018. Bull Epidémiol Hebd. 2019;(31-32):642-7.
Rahib D, Delagreverie H, Gabassi A, Le Thi TT, Vassel E, Vodosin P... & Lydié N (2021). Online self-sampling kits to screen MSM with multiple partners for HIV and other STIs: participant characteristics and factors associated with kit use in the first 3 months of the MemoDepistages program, France, 2018. Sexually Transmitted Infections, 97(2), 134-140.
In relation to

Hepatitis B and D
thematic dossier
Viral liver infections can be very severe; hepatitis B and D are transmitted through sexual contact, blood, and from mother to fetus. Vaccination and screening are the cornerstones of prevention.

Hepatitis C
thematic dossier
Hepatitis C is a viral infection primarily transmitted through blood. Screening for the disease is crucial to ensuring that infected individuals receive the treatments that can now lead to a cure.
thematic dossier
Sexually transmitted infections
Les infections sexuellement transmissibles (IST) se transmettent principalement lors des rapports sexuels. Il existe de nombreux virus ou bactéries transmissibles de cette manière.